This 49 year old man who underwent closure of an atrial septal defect (ASD) 9 years before admission complains of recurrent paroxysmal tachycardias resistant to antiarrhythmic drug therapy.
Tracings 1 and 2 were recorded during episodes of tachycardias.
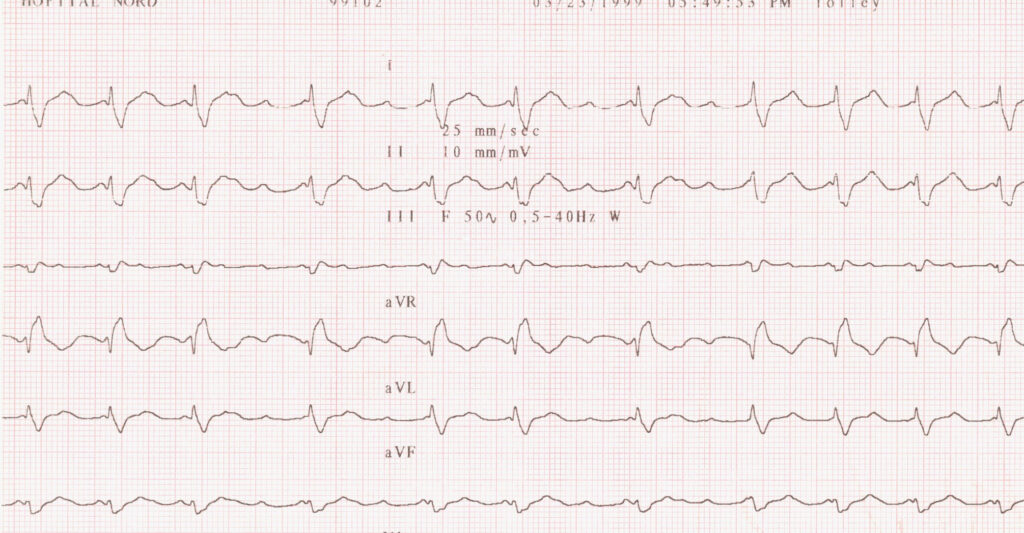
Tracing 1
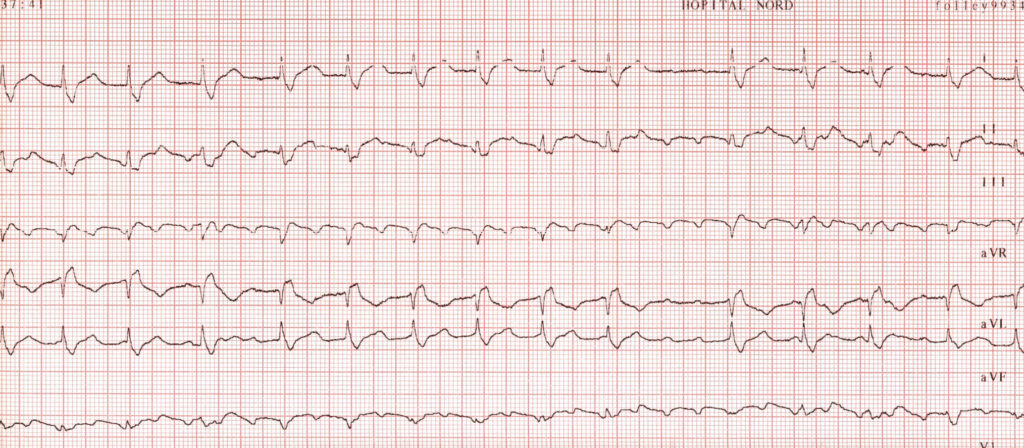
Tracing 2
Limb leads: From top to bottom 1, II, III aVF, aVL, aVF
What is your interpretation of the ECG tracings? How would you manage this case?
SEE OUR COMMENTS AND MANAGEMENT OF THIS PATIENT. CLICK HERE
Tracing 1: shows an atrial tachycardia of the atypical atrial flutter (clockwise rotation) type with positive P waves in the inferior leads (II, III and VF). The PP intervals measure approximately 300ms (200 beats per minute). Conduction to the ventricles is on the mode of the so-called alternate Wenckebach phenomenon. This phenomenon is described as 2:1 AV block at one level (lower level) of the AV node and Wenckebach of the conducted beat at the upper level terminated by 2 blocked P waves. The QRS complex has a complete right bundle branch block configuration.
Tracing 2: The P waves are fast (PP interval 280ms or 215 beats per minute) type typical counterclockwise rotation flutter (F) waves. Here again there is a 2:1 AV block as the ventricular rate is 600ms (100 beats per minute).
This atrial flutter represents a macro-reentrant atrial tachycardia which suggests in this patient with a history of surgical closure of an atrial septal defect (ASD) the so-called incisional or atriotomy macro-reentrant tachycardia rotating either around the patch or around the surgical atrial incision.
Macro-reentrant atrial tachycardia classification
Typical atrial flutter
Reversed typical atrial flutter
Atriotomy macroreentrant tachycardia
Left atrial macroreentrant tachycardia
Saoudi et al. A statement from the Working Group on arrhythmias of the ESC and of NASPE Eur Heart J 2001 and JCE 2001;12:653-9.
How to manage this patient?
1.Confirm the mechanism by performing an electrophysiologic study: The reentrant mechanism was confirmed as the tachycardia was repeatedly inducible using premature atrial stimulation
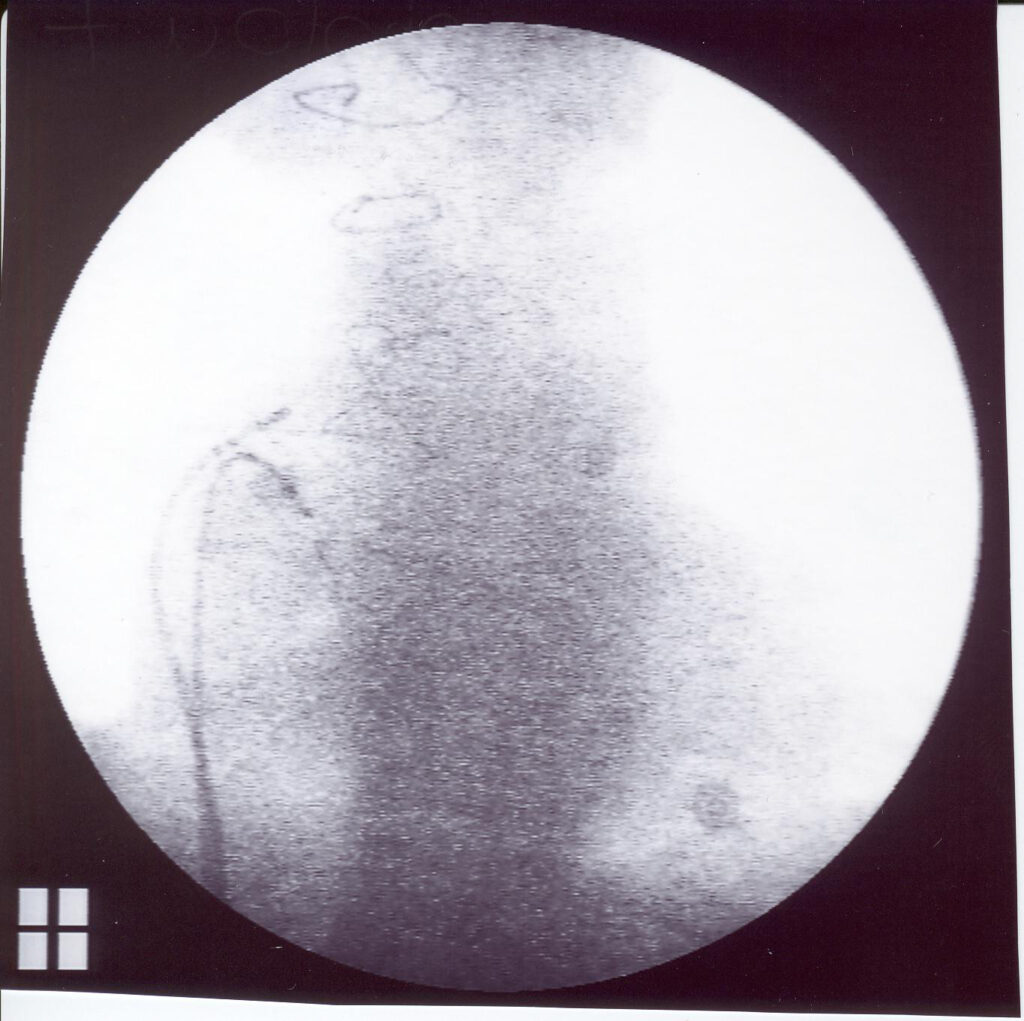
2.Perform an ablation of both tachycardias which was successfully achieved as these tachycardias were no more inducible post ablation using radiofrequency energy.
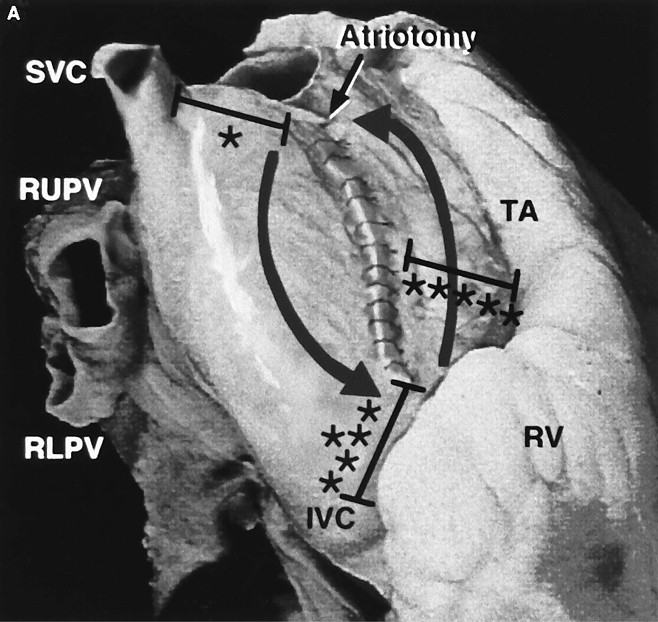
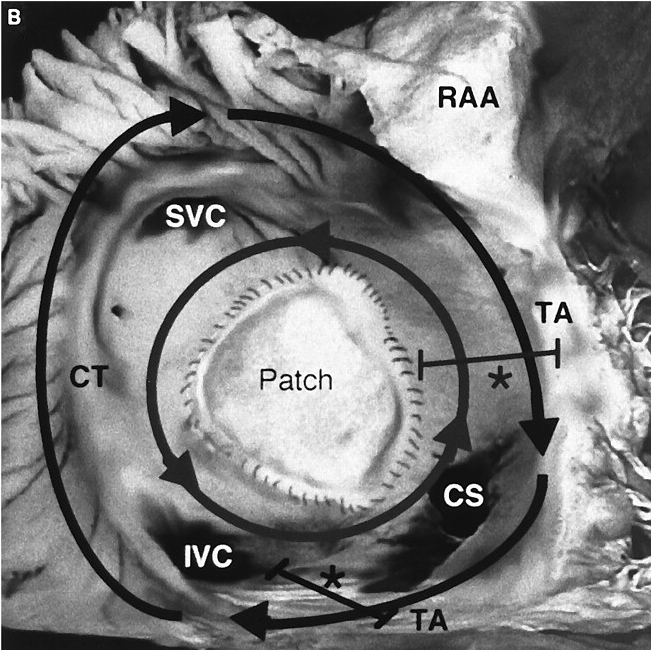
Figure 1 shows the 2 possible mechanisms of post the atrial septal defect (ASD) surgery. Right panel: circus movement around the right atrial incision. Here counterclockwise which can mimic an isthmus dependent atrial flutter and around the patch closing the ASD (Taken from the excellent paper of Kalman et al. Circulation 1996;93:502-512)
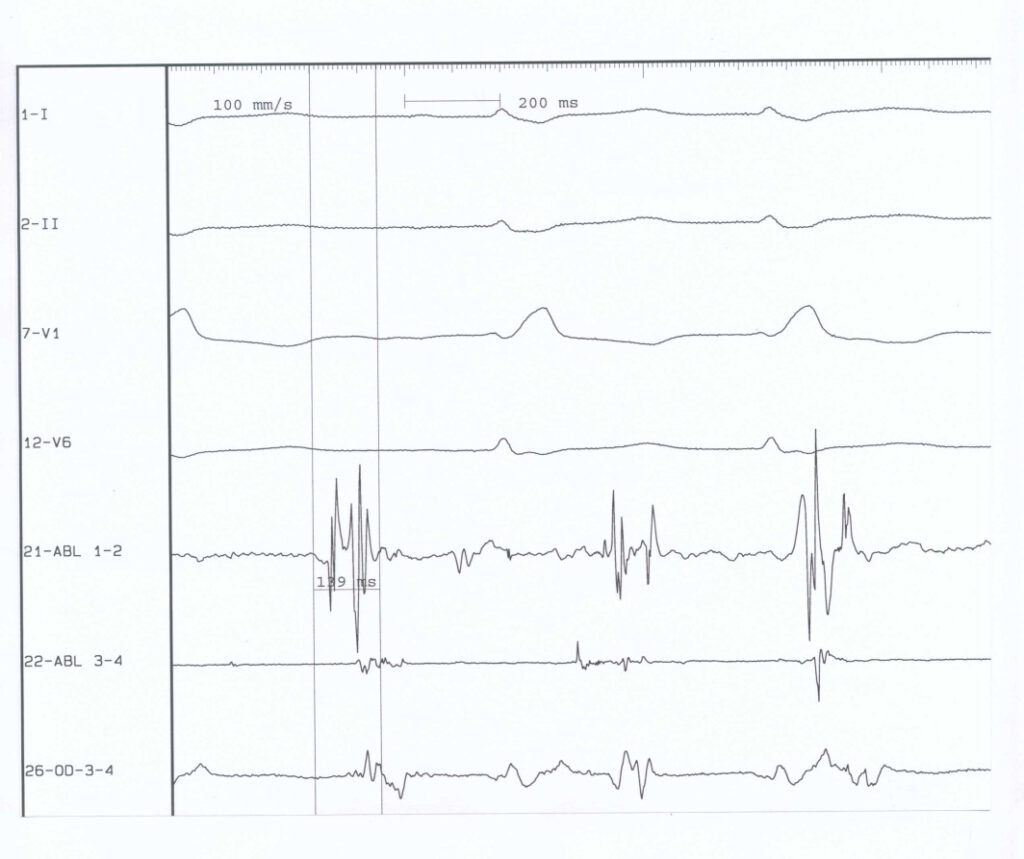
Figure 2 shows the ablation site (right panel) and the endocardial electrograms. Note the split atrial potentials at the atrial site.